Research Article submitted by:
Ramesh Manocha,1 Deborah Black,2 and Leigh Wilson2
1Discipline of Psychiatry, Sydney Medical School, University of Sydney, Royal North Shore Hospital, St. Leonards, NSW 2065, Australia
2Faculty of Health Sciences, University of Sydney, Cumberland Campus, Lidcombe, NSW 2141, Australia
Introduction
Meditation is widely perceived as an effective method of reducing stress and enhancing wellbeing. The US Centers for Disease Control and Prevention’s 2002 National Health Interview Survey administered to 31,000 representative adults showed that 8% of respondents had practiced meditation at some time. The Australian Community Survey found that 1.5 million Australians had tried meditation in the past 12 months and that while 29% of Australians found prayer to be a source of peace and wellbeing, 24% used meditation for the same thing. Remarkably, despite only about 20% of Australians attend church monthly or more often, around 33% of Australians pray or meditate at least weekly.
Health professionals are also enthusiastic about meditation despite a lack of formal education about it; a survey of Australian GPs found that almost 80% of respondents had recommended meditation to patients at some time in the course of their practice, yet less than 35% had any formal training or education in the field.
Mindfulness has become particularly popular in recent years both amongst consumers and health professionals. The growing popularity of meditation as a lifestyle and health enhancing strategy warrants more detailed assessment of its impacts on those who choose to practice it regularly over long periods of time. In spite of this, there remains a lack of evidence about the long-term health effects of regular meditation.
Despite the fact that there are hundreds, if not thousands, of interventional studies of meditation in the literature, they are limited to relatively short durations of practice, usually several weeks.
Yet meditation, as it was traditionally conceived, was intended to be a life-long practice, the benefits of which were not necessarily expected to manifest in the short term. Unfortunately, interventional studies to assess benefit (or detriment) over periods of years and decades are difficult to accomplish and are prone to a wide range of confounding effects and logistical challenges.
Meditation originated as spiritual practice in India, initially linked with Hindu spiritual philosophies such as yoga, later spread more widely in association with Buddhist spirituality to the orient. In different places, it underwent transformations giving rise to traditions such as Zen. Since the early 20th century, meditative practices, along with Eastern spiritual ideas, have become popular in the West, and in the last few decades they have become the focus of scientific attention.
Sahaja Yoga – a noncommercial form of meditation
Importantly, despite the large number of interventional studies of meditation in the literature, the vast majority are not properly designed to control for confounding, nonspecific effects. Much of this oversight relates to the lack of clarity around the definition of meditation. One definition that has yielded evidence for specific effect in rigorously designed trials is a paradigm of meditation that features the experience of “mind-emptiness” or “mental silence” as its defining characteristic .
Sahaja Yoga is a noncommercial form of meditation and is an example of this form of the mental silence approach. In this context, the meditative experience is a state in which the practitioner is fully alert, aware, and in control of their faculties but does not experience any unwanted thought activity.
Practitioners describe the experience of thoughtless awareness or “mental silence” as an enhancement of awareness and self-control, enabling them to attend to the demands of the present moment . Studies of the mental silence approach to meditation have been conducted in a range of health conditions .
Rigorous randomised trials using active control groups have demonstrated significant effects on mood and airway hyperresponsiveness in asthma sufferers and on depressive mood and work stress in full-time workers.
In other studies, promising effects have been shown in depression/anxiety , attention deficit and hyperactivity disorder , menopausal hot flashes, and epilepsy. Brain physiological studies indicate that the meditative experience is highly correlated with specific electrical activation patterns.
Discussion
It is important to note that while modern science most commonly characterises meditation as a relaxation response or a pattern of specifically focused attention, these conceptualisations differ fundamentally from the authentic descriptions of the meditative experience originating in ancient India. The original source texts clearly state that a key defining feature of meditation is the experience of mental silence.
For example, in what is probably the oldest known definition of meditation, the narrator explains in the ancient Indian Mahabharata that a meditator is “… like a log, he does not think” . Similarly Lao Tse instructs the reader in the Tao Te Ching to “empty the mind of all thoughts”. Many other explicit examples of this idea can be found in Eastern literature from virtually every historical period. Yet Western definitions of meditation have consistently failed to acknowledge this crucial feature.
The mechanisms by which meditation techniques exert their claimed effects are also unclear. One very popular view, which has become more or less the default explanation, is that the physiological changes are characterised by the relaxation response—that is, the physiological changes that occur during rest, characterised by reductions in heart rate, blood pressure, and respiratory rate and increases in skin temperature, skin resistance, and alpha wave activity in the brain are thought to be responsible.
All of these are brought about by reducing activity of the sympathetic component of the autonomic nervous system and increasing activity of the parasympathetic components of the ANS. Psychophysiological studies of Sahaja Yoga, that is mental silence, however suggest that it does not elicit a typical relaxation response.
For example, a study of skin temperature changes during a single Sahaja Yoga meditation session demonstrated a reduction in palmar skin temperature, which is the opposite of that predicted by the relaxation response model. A control group that was engaged in simple rest did manifest skin temperature increases. Yet there were no significant differences in heart rate between the two groups .
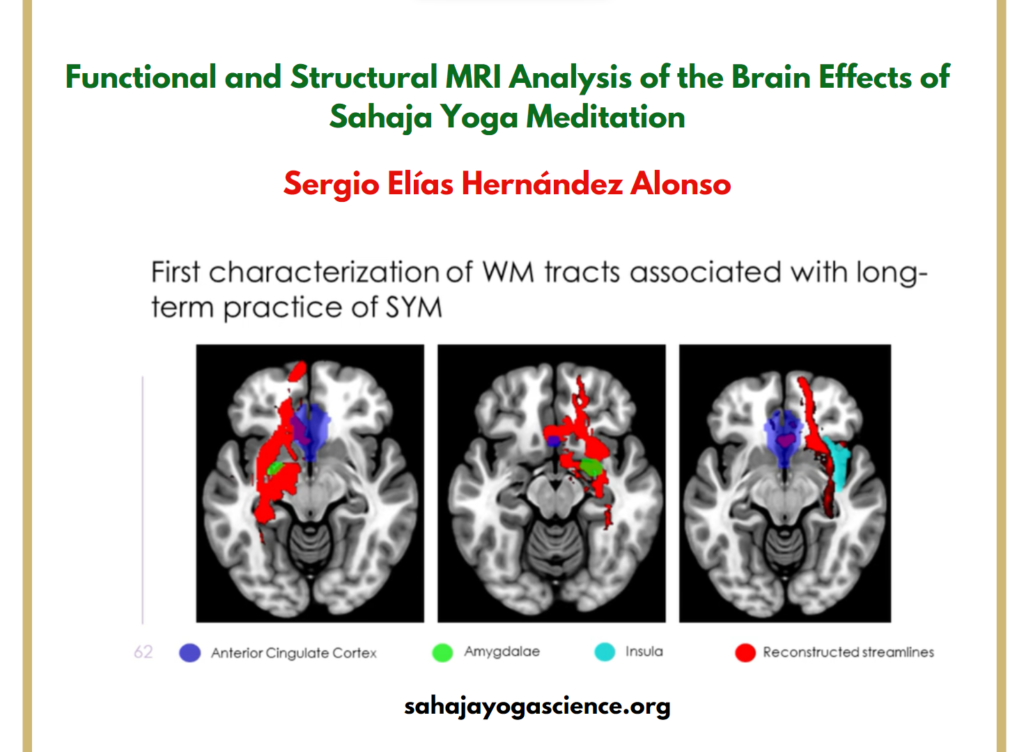
Meditation can have short- and long-term effects on both function and structural brain plasticity
There is evidence that meditation can have short- and long-term effects on both function and structural brain plasticity in addition to its already recognised ability to cause relaxation and reduce stress. Aftanas has shown that the practice of Sahaja Yoga meditation, and the experience of mental silence, is strongly reflected in both brain electrophysiology and mood .
A study by the same group demonstrated reduced emotional reactivity in long-term meditators compared to controls which was reflected in psychological, physiological, and electrophysiological reactivity to standardised stressful stimuli presented in a video film. This provides evidence for the notion of “emotional detachment” and hence enhanced emotional stability and resilience to stressful events .
A smaller intervention study by Morgan over just 6 weeks showed a significant reduction in anxiety, depression, and related symptoms in patients with major depression compared to controls [17] which appears to reflect the clinical relevance of Aftanas’s findings. This has broader implications particularly as understandings of the relationship between neuroplasticity and meditation emerge.
Lazar studied a group of Buddhist meditators and found that meditators compared to controls had significantly increased cortical thickness in right middle and superior frontal cortex and insula suggesting that meditation is associated with delaying of the usually age-related thinning of right frontolimbic brain regions . Hence it is quite possible that long-term meditation may facilitate both electrophysiological and structural changes in brain function that may explain why the population of long-term meditators that we studied manifested an apparent advantage as compared to the background population particularly in metal health scores.
Conclusion
This is the first study to report a cross-sectional survey aimed at assessing health and quality of life in a population of people who meditate regularly and have done so for a long period of time. It is also the first study to explore the interrelationship between factors such as meditative experience, meditative practices, a “meditative” lifestyle, and health outcomes.
Long-term Sahaja Yoga meditation practitioners appear to experience better quality of life and functional health than the general population. Perhaps most importantly is the observation that there appears to be a relatively robust and consistent relationship between the meditative experience of mental silence and health, especially mental health.
Based on the premise and findings of this study, these observations necessarily apply to practitioners of mental silence-orientated forms of meditation of which Sahaja Yoga is an example. Taking into account the fact that two well-designed RCTs of mental silence also demonstrated significant effects on both mental and physical health parameters compared to active controls, the association between the subjectively reported experience of mental silence and health observed in this study is likely to be causal. Hence this survey data suggests that such approaches to meditation may have a potentially valuable role in primary mental health prevention. Further research to evaluate this possibility is clearly warranted.
Future research involving comparison of mental-silence-orientated practitioners with other populations (controlling for the exclusion of health risk factors and similar lifestyle changes as well as religious and spiritual observances) would be useful to more clearly identify the source of the apparent benefits of that this population appears to enjoy.
Read entire article – https://www.hindawi.com/journals/ecam/2012/350674/